The excess mucus and inflammatory cells produced by the lungs can be observed in the lower trachea and a sample collected (via ‘tracheal wash’) for analysis. Respiratory secretions can also be collected from the small airways using a technique called a ‘lung wash’ or ‘bronchoalveolar lavage’. During disease remission these secretions and their cellular content return to normal.
Asthma can be prevented if the causative allergens are known. For example, a horse with allergens in the stable environment can often be kept in remission by avoiding hay and straw. If this isn’t possible and you’re feeding hay or haylage then high temperature steaming is an effective way to reduce airborne respirable dust and allergens prior to feeding. Find out more about high temperature steaming - CLICK HERE. For horses with field-based allergens, this is far harder as the allergens are difficult to determine and are often very hard to avoid. Once diagnosed, the horse will always be susceptible to asthma; the disease is managed not cured. It is best to prevent asthma rather than need to treat it with drugs. If good environmental management cannot be maintained, treatment with oral or inhaled steroids and/or bronchodilators may be required.
• Pneumonia / Pleuropneumonia
Bacterial infection of the lungs (pneumonia) is most commonly seen in foals where Rhodococcus equi is the most common cause. In adult horses, pneumonia can occur following an episode of oesophageal obstruction (‘choke’) where food material and saliva have been accidentally aspirated or following long travel. Journeys of over 6h are a known risk factor for pleuropneumonia, a serious condition where bacterial infection of both the lungs and chest cavity occurs. Horses present with fever, cough, nasal discharge, increased respiratory rate and, with pleuropneumonia, may also show reluctance to move. Diagnosis is via ultrasonography of the chest to identify lung abscesses, collapsed lung lobes and the presence of fluid in the chest cavity. Treatment requires intensive care, intravenous antibiotics with additional drainage of any infected chest fluid present (Fig. 5), and is not always successful.
• Equine Mulitinodular Pulmonary fibrosis
Recently equine herpesvirus 5 has been identified as the cause of a fibrotic lung disease caused equine multinodular pulmonary fibrosis (EMPF). Horses present with severe respiratory distress, intermittent fever, cough, nasal discharge, decreased appetite, weight loss, thin body condition and lethargy. This disease is rare but can be identified by PCR and lung biopsy. Some response is reported to antiviral medication but most horses require euthanasia.
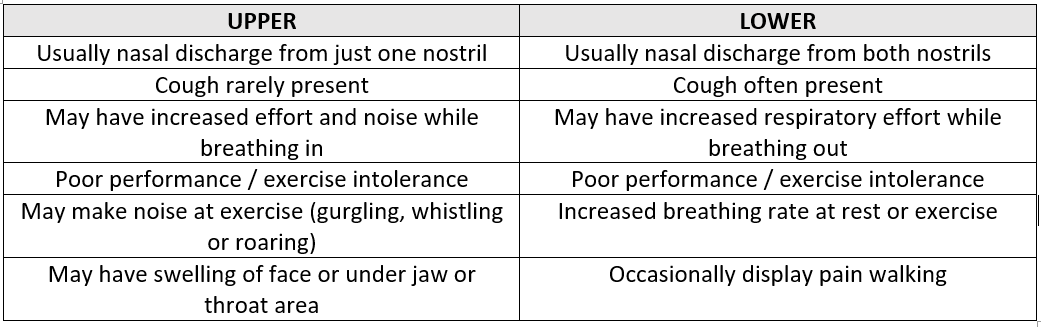
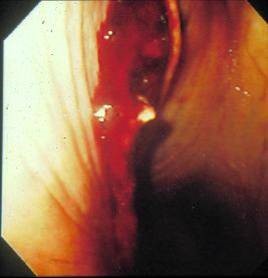
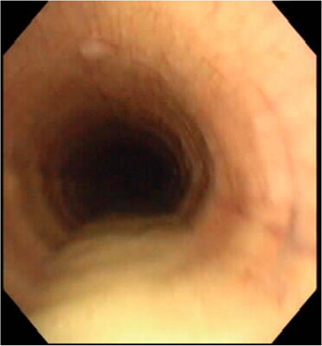
• Foreign body
Inhalation of a foreign body, e.g. a stick, can be a rare cause of a snotty nose (Fig. 6). Usually endoscopic removal can be performed with antibiotic treatment of any secondary bacterial infection.